What is the role of nasogastric lavage in diagnosing GI bleeding?
What is the role of nasogastric lavage in diagnosing GI bleeding?
Nasogastric lavage may confirm recent upper gastrointestinal (GI) bleeding (UGIB) (coffee ground appearance), possible active bleeding (red blood in the aspirate that does not clear), or a lack of blood in the stomach (active bleeding less likely but does not exclude an upper GI lesion).
What is NGT lavage?
Abbreviation: NG (nasogastric) Nasogastric (NG) lavage is an intuitively logical procedure for evaluation of the patient suspected of having acute upper GI bleeding. Indeed, a bloody NG aspirate is a good predictor of finding a high-risk lesion on upper endoscopy.
What is the ICD 9 code for GI bleed?
ICD-9-CM Diagnosis Code 578.9 : Hemorrhage of gastrointestinal tract, unspecified.
What is the treatment for an upper GI bleed?
If you have an upper GI bleed, you might be given an IV drug known as a proton pump inhibitor (PPI) to suppress stomach acid production. Once the source of the bleeding is identified, your doctor will determine whether you need to continue taking a PPI .
Why do NG tubes bleed?
Traumatic injury to the GI mucosa may occur during NG tube insertion and can result in GI bleed, especially in patients with coagulopathy. Prolonged use of NG tube can cause ulcer formation due to continuous irritation and pressure necrosis.
What is GI bleeding?
Gastrointestinal (GI) bleeding is a symptom of a disorder in your digestive tract. The blood often appears in stool or vomit but isn’t always visible, though it may cause the stool to look black or tarry. The level of bleeding can range from mild to severe and can be life-threatening.
How do you perform nasogastric lavage?
- Insert the nasogastric/orogastric tube into the stomach, then confirm placement (see Nasogastric/Orogastric Tube Insertion).
- Introduce 200 to 300 mL of water at body temperature into the tube and then lower the tube into the bucket below the level of the stomach before water disappears from the funnel.
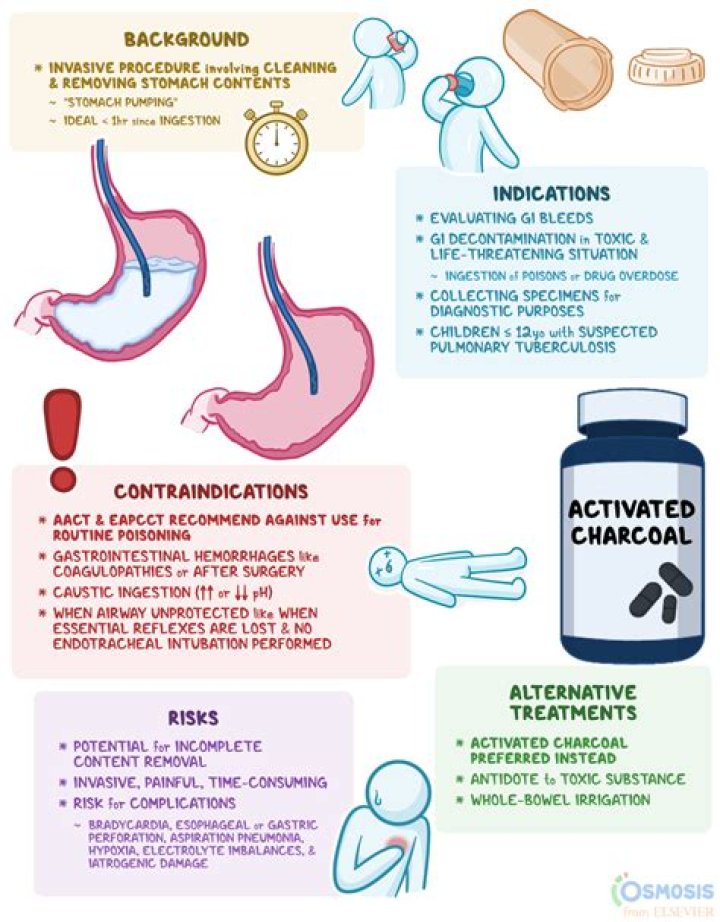
What is gastric lavage indication?
Indications. Life-threatening poisoning (or history is not available) and unconscious presentation (eg Colchicine) Life-threatening poisoning and presentation within 1 hour. Life-threatening poisoning with drug with anticholinergic effects and presentation within 4 hours.
What is ICD-10 code for GI bleed?
Gastrointestinal hemorrhage, unspecified K92. 2 is a billable/specific ICD-10-CM code that can be used to indicate a diagnosis for reimbursement purposes.
What is the difference between upper and lower GI bleed?
Upper GI bleeding: The upper GI tract includes the esophagus (the tube from the mouth to the stomach), stomach, and first part of the small intestine. Lower GI bleeding: The lower GI tract includes much of the small intestine, large intestine or bowels, rectum, and anus.
Can a feeding tube cause internal bleeding?
A rare, and often unrecognized, complication of gastrostomy tube placement is upper gastrointestinal bleeding secondary to a gastric ulcer caused by pressure from a gastrostomy tube bumper or balloon. Here, we present a case of an elderly woman who experienced hematemesis and bleeding around the gastrostomy site.
What does a nasogastric lavage show?
Nasogastric lavage may confirm recent upper gastrointestinal (GI) bleeding (UGIB) (coffee ground appearance), possible active bleeding (red blood in the aspirate that does not clear), or a lack of blood in the stomach (active bleeding less likely but does not exclude an upper GI lesion).
What is the role of nasogastric (NG) tubes in GI bleeding?
NG tubes have been used for various reasons in patients with GI bleeding. In the past, NG lavage was thought to help control GI bleeding. However, recent studies have shown that this is not helpful. Another indication for placement of a nasogastric tube is in the setting of massive hematochezia.
What is the role of nasogastric tube placement in massive hematochezia?
Given that up to 15% of massive hematochezia is caused by an upper GI bleed, placement of a nasogastric tube, after initiating resuscitation may potentially aid in diagnosis. Of note, an upper GI source of bleeding is only ruled out after aspiration of gastric contents from a nasogastric tube if the fluid is bile tinged.
Is nasogastric tube placement contraindicated in patients with esophageal varices?
A nasogastric tube is an important diagnostic tool, and tube placement can reduce the patient’s need to vomit. Placement for diagnostic purposes is not contraindicated in patients with possible esophageal varices.